
What is EMDR?
EMDR stands for Eye Movement Desensitisation & Reprocessing. It is a psychotherapeutic procedure that was originated and developed by Dr Francine Shapiro in the United States in 1987.
EMDR was originally designed to treat traumatic or “dysfunctional” memories and experiences and their psychological consequences, and the procedure has mainly been used in the treatment of Post stress traumatic syndrome.
However EMDR has been increasingly used over the years to treat e.g., grief, phobias, test and performance anxiety, anxiety and panic disorders, pain, sexual dysfunction, and a wide range of experientially based disorders.

EMDR is an evidence based therapeutic procedure. That is, although the procedure originally developed out of self-observation, the evolution and development of the procedure has been dictated by clinical and research findings.
Most of the components in EMDR are recognisable from other well-known therapies although they are arranged in a unique order. However, one unusual element in EMDR is bilateral stimulation usually in the form of eye movements, but also sometimes in the form of bilateral auditory or tactile stimulation.

There is a great deal of evidence that bilateral stimulation speeds up the reprocessing of disturbing emotional or traumatic material and at the same time helps the client feel safer in making contact with traumatic material. A number of replicated research trials have demonstrated that eye movements reduce the vividness of emotional and traumatic imagery.
It is believed that the eye movements induced in EMDR mirror the natural eye movement process that occurs in the REM (Rapid Eye Movement) phase of sleep during which information is processed naturally.
In EMDR, the therapist will always firstly carry out a careful psychological assessment of whether EMDR would be suitable for the problem (s) presented, and will elicit a memory representing the problem.
The client will be asked for a picture that represents the memory, a negative belief that they have about themselves in relation to the memory, and to notice associated physical sensations. Thereafter, a number of sets of eye movements or other bilateral stimulation are commenced, and after each set of eye movements the therapist will ask the client what they noticed.

Typically, the images, emotions, and sensations experienced change through this process. At some point these changes become more positive and adaptive as the clientreprocesses old dysfunctional information and connects with presently held adaptive and functional information. The aim is always to enable the client to recollect the original traumatic material without disturbance and to have new and more adaptive beliefs about themselves in relation to the experience.
With “simple” or “one off” traumas or experiences in adult life, EMDR can be remarkably rapid in its effects, and average treatment times for these kinds of problems are from 3 to 5 sessions. With more “complex” or multiple traumas treatment can take much longer but the evidence that we have to date suggests that EMDR is the most efficient and rapid psychotherapeutic procedure available for the treatment of traumatic memories and Post Traumatic Stress Disorder.
However treatment should only be untaken with a therapist properly trained and preferably accredited.
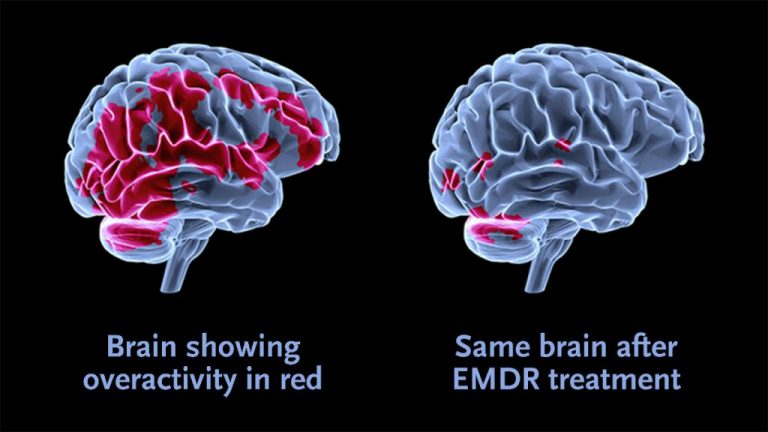
(FMRI image that shows pre-post EMDR therapy)
**********************************************
CONTACTS in MILAN – ITALY
Dr. Martina Larsen Payà +39 349 1696270
**********************************************

 LOCKED IN THE HOUSE")


